
Past Performance Not Indicative of Future Results
Negative experiences lead nearly 50% of families of kids with disabilities to leave their church. But there’s a roadmap for overcoming past experience for families raising kids with mental illness.


The final barrier we’re going to examine in this series looking at why families of kids with mental health issues are missing from church has to do with the family’s past experiences of church. For many who have sought to attend church as a family, their experiences resulted in they or their children feeling anxious, misunderstood, lonely, isolated, drained or judged.
As we consider how we might strategize coming alongside families in overcoming past experiences of church, it’s helpful to look at some very new research examining this concern among families of children served by disability ministry.
If you have a significant interest in disability inclusion as a pastor, ministry leader and a parent, I would strongly encourage you to watch the video posted below from beginning to end of Dr. Erik Carter’s talk presented at our ministry’s Disability and the Church conference this past April. This is probably the most important original research ever presented at one of our conferences and was derived from a study conducted by his Baylor University team with 350 families raising children with disabilities recruited from churches across Texas.
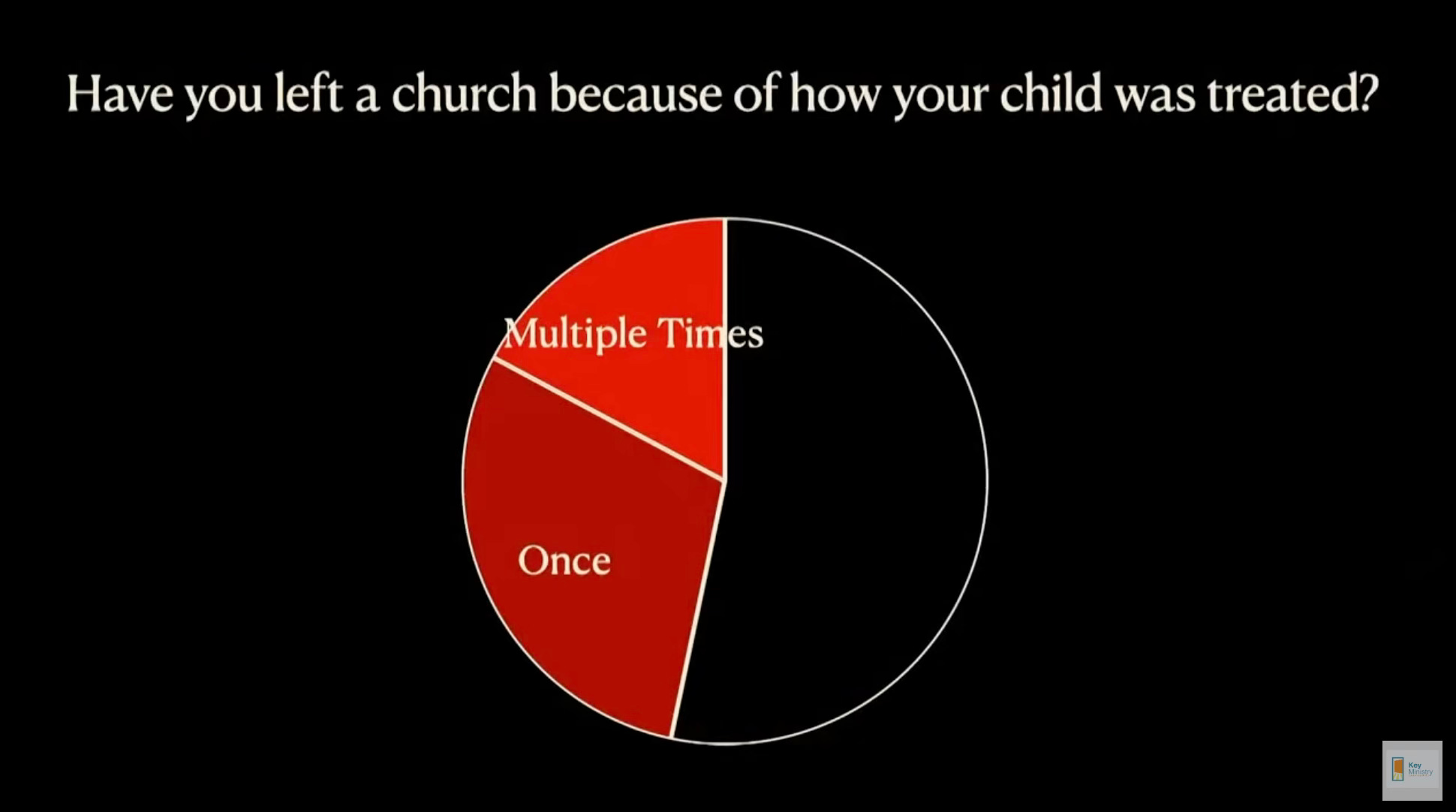
In this study, 48% of families reported having left a church as a result of how their child had been treated. I can’t say I was surprised. While not a representative sample, 60.7% of the 541 registrants for our ministry’s 2014 Web Summit reported having to leave church as a result of their own, or a family member’s disability.
A large subset of those families in Dr. Carter’s study - approximately 20% of the overall sample reported leaving multiple churches as a result of how their kids were treated. And yet, ALL of them were actively connected with a church at the time they were interviewed as a function of the study design.
What was most telling were the differences in experience parents reported for themselves and their children engaged in churches with an identified disability ministry. In the two graphs below, bars in green describe the experiences of parents, or parent reports of their child’s experience of church in churches with an identified disability ministry, with the bars in red representing churches without a disability ministry.
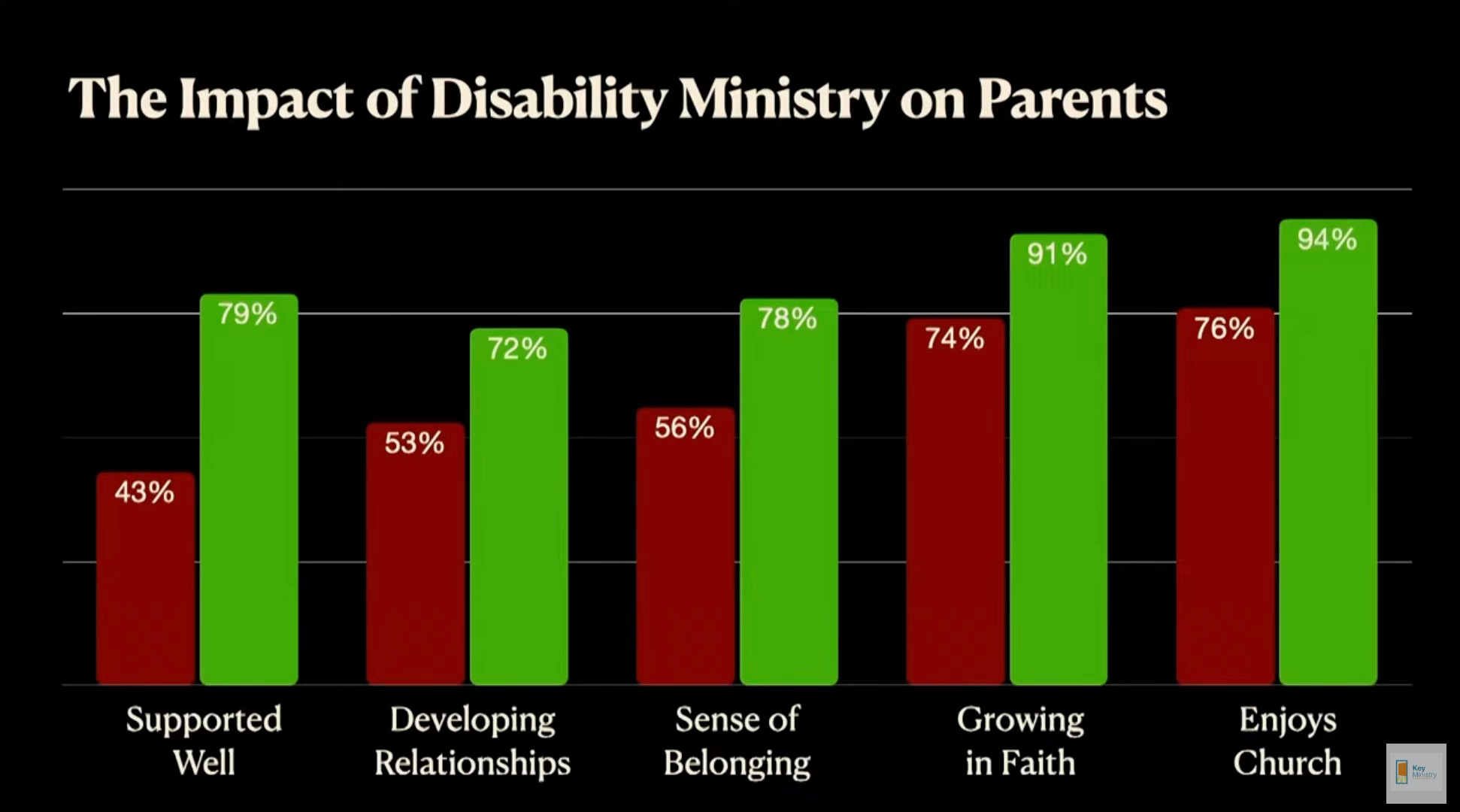
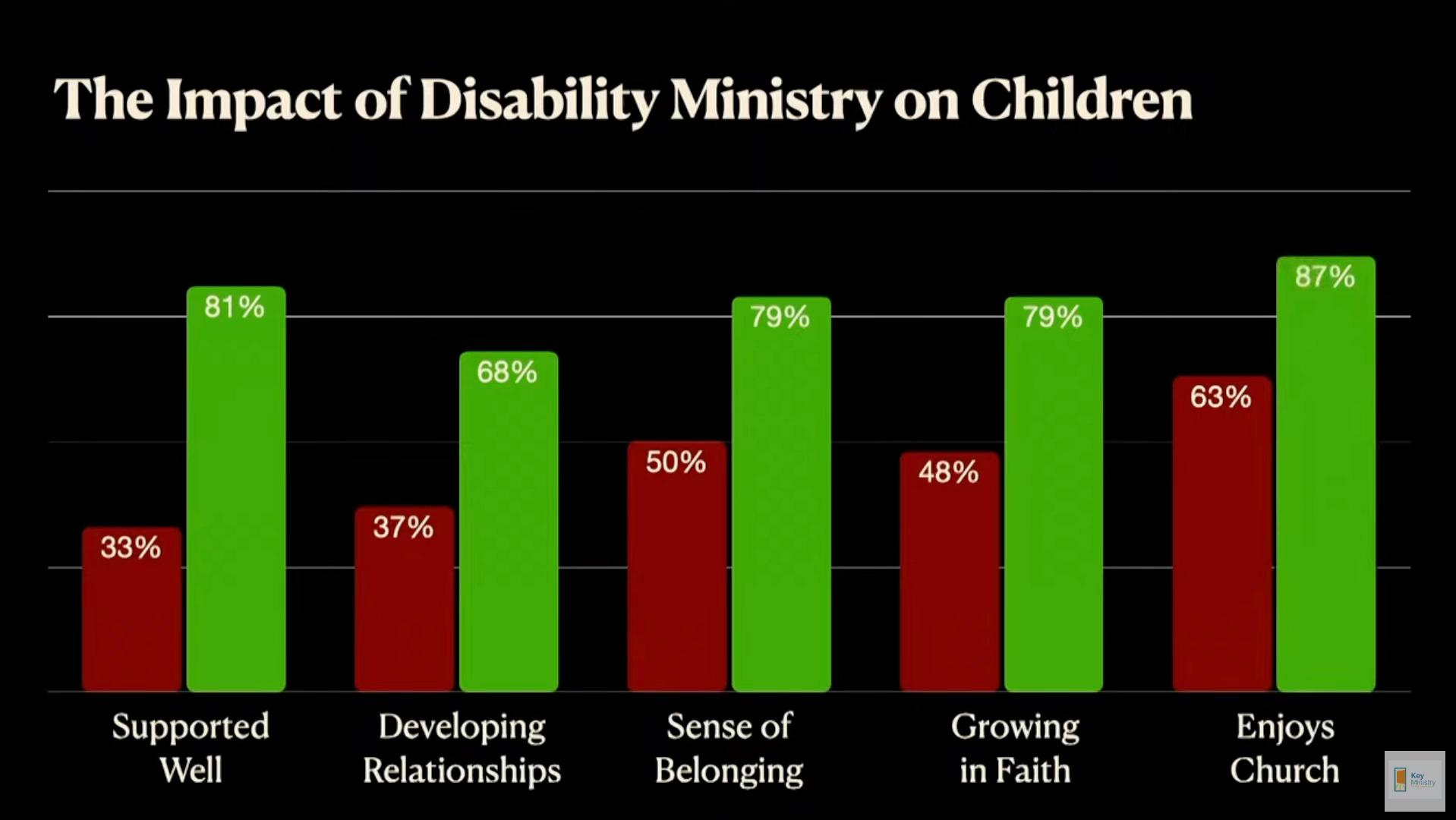
Churches that are intentional in wanting to provide the supports, create the spaces and make the accommodations appropriate for welcoming families of kids with disabilities had a great impact. One would think that by creating ministries addressing the inclusion and support needs of kids with common mental health conditions we would see similar results. But there are significant differences between families raising kids with mental health conditions and those raising kids with intellectual or developmental disabilities (mental health conditions seemingly having a greater impact on church attendance) that may impact the fruitfulness of inclusive mental health ministry or necessitate different approaches with mental health inclusion.
One difference between disabilities that are typically the focus of “special needs” ministries and mental health disabilities is the multigenerational expression of many common mental health conditions. I learned pretty quickly in my child psychiatry training that the apple doesn’t fall far from the tree and my kids with mental health issues often had parents who also had issues. Some mental health conditions are highly heritable. Roughly one in three children of parents who have schizophrenia, bipolar disorder, or depression will develop a serious mental illness—and not necessarily the same mental illness as their parent. A parental history of anxiety (especially maternal history) contributes to a twofold to sevenfold increase in the risk for anxiety in their offspring.
As a result, any strategies to include kids with mental illness at church must also address the obstacles a child’s parents or caregivers may experience in association with their own mental health issues. After all, if Mom or Dad doesn’t attend church, it’s highly unlikely that their kids will be coming to church. This may be one explanation for why mental health conditions are more likely to impact church attendance than intellectual or developmental disabilities. Adults who have children with “special needs” typically don’t need accommodations to attend church themselves. That may not be the case for parents of kids with mental health challenges.
Another striking finding from Dr. Carter’s study that may not generalize to the same extent in families raising kids with mental illness is the extraordinary importance the parents placed upon the involvement of their children at church. 99% reported church participation as “important” or “very important” for their child with a disability.

When a parent raised with a strong faith in Christ has a bad church experience resulting from the church’s response to a child with a disability, it appears from Dr. Carter’s research that families will often seek another church better prepared to address their child’s needs. But what happens when a parent who hasn’t yet come to value a positive church experience so highly experiences a problem at church related to their own, or a family member’s mental health challenges? For them to give church another try, they’ll likely need to be convinced their next experience will be different.
What conclusions can we draw from Dr. Carter’s research for families raising kids with mental health disabilities when it comes to church attendance?
Parents for whom personal faith and their child’s ability to be involved with church is important will persist in looking for a church where every member of the family can have a positive experience.
Churches that offer appropriate supports for mental health inclusion are likely to have impacts similar to churches with identified disability ministries.
Including children with mental health challenges likely to persist in some form into adulthood at church is critically important given the multigenerational impact of these conditions on church attendance.
If you’re interested in learning more about what churches can do in formulating a strategy for outreach to and inclusion of the mental health community, I’d encourage you to read Mental Health and the Church. If you’re a pastor or church staff member interested in implementing mental health ministry, I’d encourage you to reach out to our team at Key Ministry for free consultation tailored to your church’s unique needs.